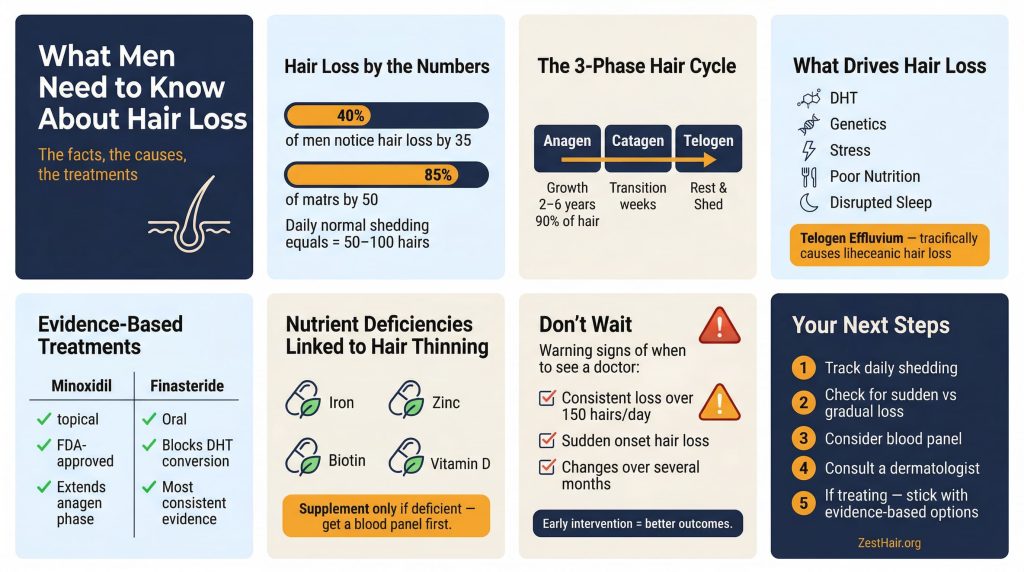
By your mid-thirties, there’s a reasonable chance you’ve already started thinking about your hair differently. Not because you’re vain — because the numbers are real. Around 40% of men notice meaningful hair loss by 35. By 50, that figure climbs to roughly 85%. This isn’t a rare condition. It’s a predictable biological process, and understanding it puts you in a much better position than panic or denial.
Your Hair Is Always Shedding — That’s the Baseline
The average person loses between 50 and 100 hairs per day. Given that a healthy scalp holds around 100,000 follicles, that daily loss is unremarkable. The concern isn’t shedding — it’s shedding without adequate regrowth.
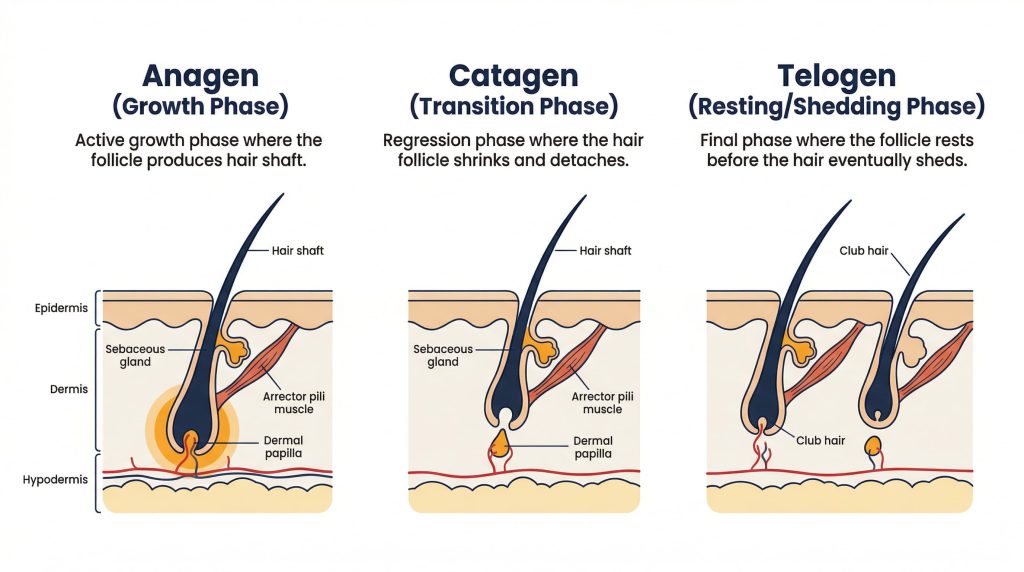
Hair operates on a three-phase cycle. The anagen (growth) phase lasts two to six years and accounts for roughly 90% of your hair at any given moment. After that, a short catagen (transition) phase lasts a few weeks, followed by the telogen (resting) phase, after which the hair sheds and the cycle starts again.
When that cycle gets disrupted — shortened growth phases, weakened follicles, or hormonal interference — you lose more than you replace. That’s when thinning becomes visible.
What this means for you: Losing hair on your pillow or in the shower isn’t automatically a red flag. If you’re consistently losing well over 150 hairs a day, or noticing changes in density and hairline, that’s worth paying attention to.
What Actually Drives Hair Loss
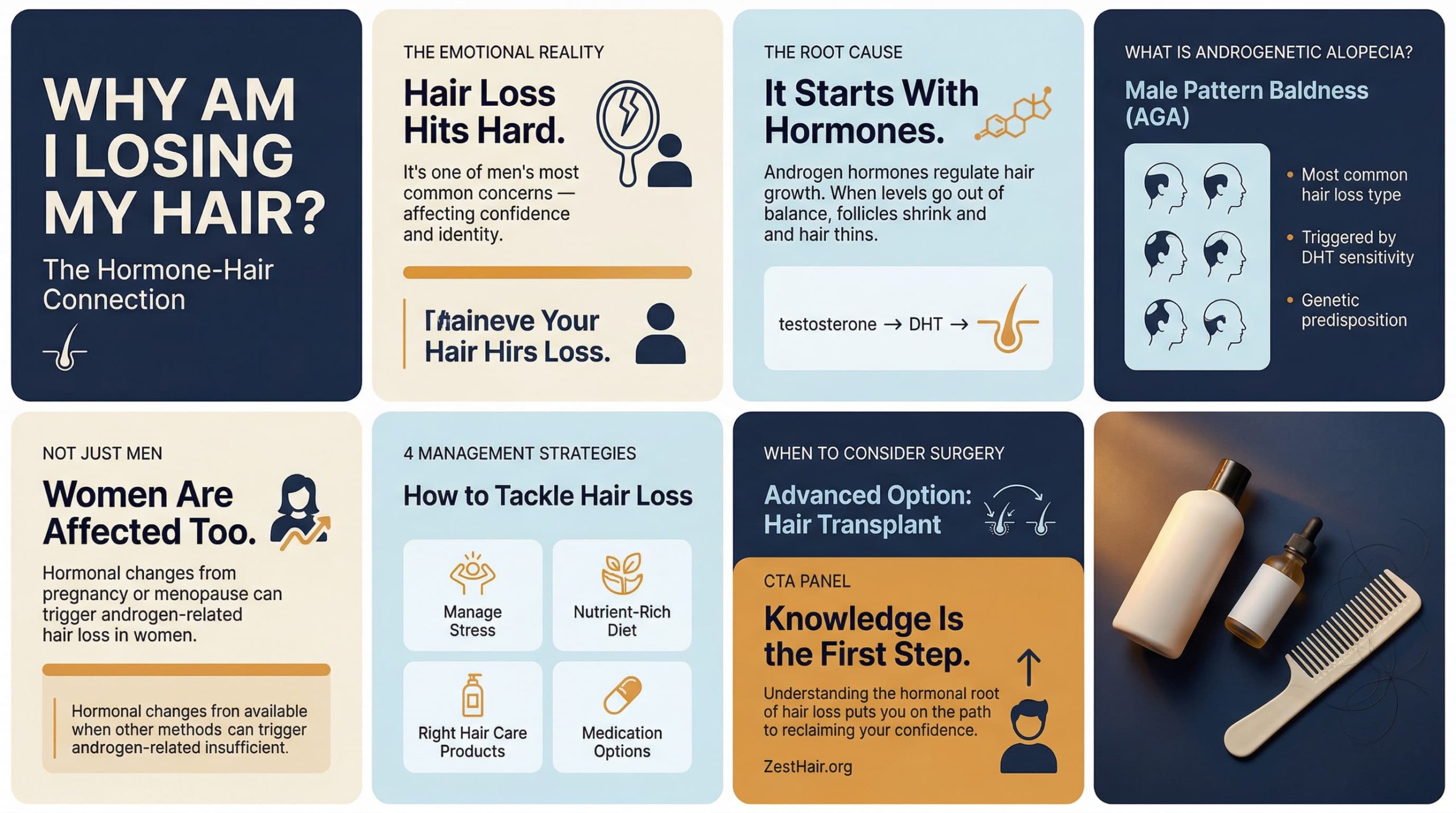
The most common cause in men is androgenetic alopecia — male pattern baldness. It’s driven primarily by DHT (dihydrotestosterone), a derivative of testosterone that binds to hair follicles and gradually shrinks them over time. Genetics determine how sensitive your follicles are to DHT, which is why some men are mostly bald in their twenties while others keep a full head well into their sixties.
But genetics isn’t the only factor. Research consistently links accelerated hair loss to stress, poor nutrition, disrupted sleep, and certain medications. A condition called telogen effluvium — where a significant number of follicles are pushed into the resting phase simultaneously — can cause rapid, temporary shedding in response to illness, crash diets, surgery, or intense psychological stress. It’s reversible in most cases, but it can be alarming if you don’t know what’s happening.
Hormones beyond DHT — including thyroid hormones and cortisol — also play a documented role. An underactive thyroid, for example, is a well-known cause of diffuse hair thinning.
What this means for you: If your hair loss came on suddenly rather than gradually, or if it’s accompanied by other symptoms like fatigue or skin changes, see a doctor rather than going straight to the supplement aisle. Sudden hair loss has specific causes worth identifying.
What the Evidence Says About Prevention and Treatment
This is where most of the noise is, so it helps to be specific about what actually has clinical backing versus what’s largely marketing.
Minoxidil (sold as Rogaine) is an FDA-approved topical treatment that works by prolonging the anagen phase and improving blood flow to follicles. Research shows it’s effective for many men, particularly when started early. It doesn’t work for everyone, and it requires ongoing use — stopping it reverses the benefit within months.
Finasteride is an oral medication that blocks the conversion of testosterone to DHT. It’s one of the more effective options for androgenetic alopecia, with studies showing it slows or halts progression in the majority of users. It carries potential side effects — including, in a minority of cases, sexual dysfunction — which are worth discussing with a physician before starting. For a more detailed breakdown, the hair loss medications guide on this site covers what the science actually supports.
On the nutritional side, deficiencies in iron, zinc, biotin, and vitamin D have all been linked to hair thinning in clinical research. The key word is deficiency — supplementing these nutrients when you’re already at normal levels generally doesn’t produce noticeable results. A blood panel is more useful than a shopping trip. The seven essential nutrients for hair growth piece breaks this down in more detail.
What this means for you: Minoxidil and finasteride are the two treatments with the most consistent evidence behind them. Everything else — laser combs, exotic shampoos, DHT-blocking supplements — has either weak evidence or no evidence at scale. That doesn’t mean none of it works, but don’t let aggressive marketing substitute for efficacy data.
![]()
When to See a Professional
Most men wait too long. By the time hair loss is obvious to others, significant follicle miniaturisation has often already occurred. Follicles that have fully stopped producing hair are generally not recoverable with current treatments — which is why early intervention matters.
A dermatologist or trichologist can assess whether you’re dealing with androgenetic alopecia, a nutrient deficiency, a hormonal condition, or something else. They can also evaluate whether what you’re doing is actually working. If you’re considering treatment, that assessment is worth more than any off-the-shelf product.
What this means for you: If you’ve noticed consistent changes in your hairline, density, or daily shedding over several months, make the appointment. A clinical evaluation is low cost relative to months of trial-and-error with products.
The Psychological Weight Is Real — And Underreported
Hair is tied to identity and self-perception in ways that most people don’t examine openly. Research in this area confirms what most men already know privately: hair loss can affect confidence, social behaviour, and mental wellbeing. That’s not weakness — it’s a documented psychological response to a visible change in appearance.
What’s worth separating is the distress from the threat. Hair loss is not a health emergency for most men. It doesn’t affect lifespan, physical capability, or cognitive function. But if it’s affecting your confidence or how you carry yourself in professional or social contexts, that’s a legitimate concern — and there are both practical (treatment, styling) and psychological routes to address it. The hair loss psychology guide covers this more thoroughly if you’re dealing with the mental side of it.
What this means for you: There’s no obligation to be indifferent about losing hair. Acknowledge how it affects you, then make informed decisions about what, if anything, you want to do about it.
What to Take Away
Hair loss in men is largely predictable, often treatable when caught early, and almost never as catastrophic as it feels in the moment. The key points:
- Daily shedding of 50–100 hairs is normal. Consistent loss above ~150/day warrants attention.
- Most male hair loss is DHT-driven and genetic, but stress, nutrition, sleep, and hormones all contribute.
- Minoxidil and finasteride are the treatments with the strongest evidence base. Most other options are less proven.
- Early intervention produces better outcomes than waiting.
- If the pattern or speed of loss concerns you, a dermatologist is the right first stop — not a supplement stack.
The decision you’re actually facing is straightforward: gather accurate information, assess where you are, and choose how you want to respond. That’s it.